Cartilage doesn't heal. Once it's gone — worn down by arthritis or damaged by injury — the body has essentially no mechanism to regenerate it. That's why osteoarthritis, which affects more than 500 million people globally, has no disease-modifying treatments. Current options manage pain; none actually fix the joint.
A remarkable paper in Science (2025/2026) from Stanford suggests that might be about to change — and a lipid-signaling enzyme is at the center of the story.
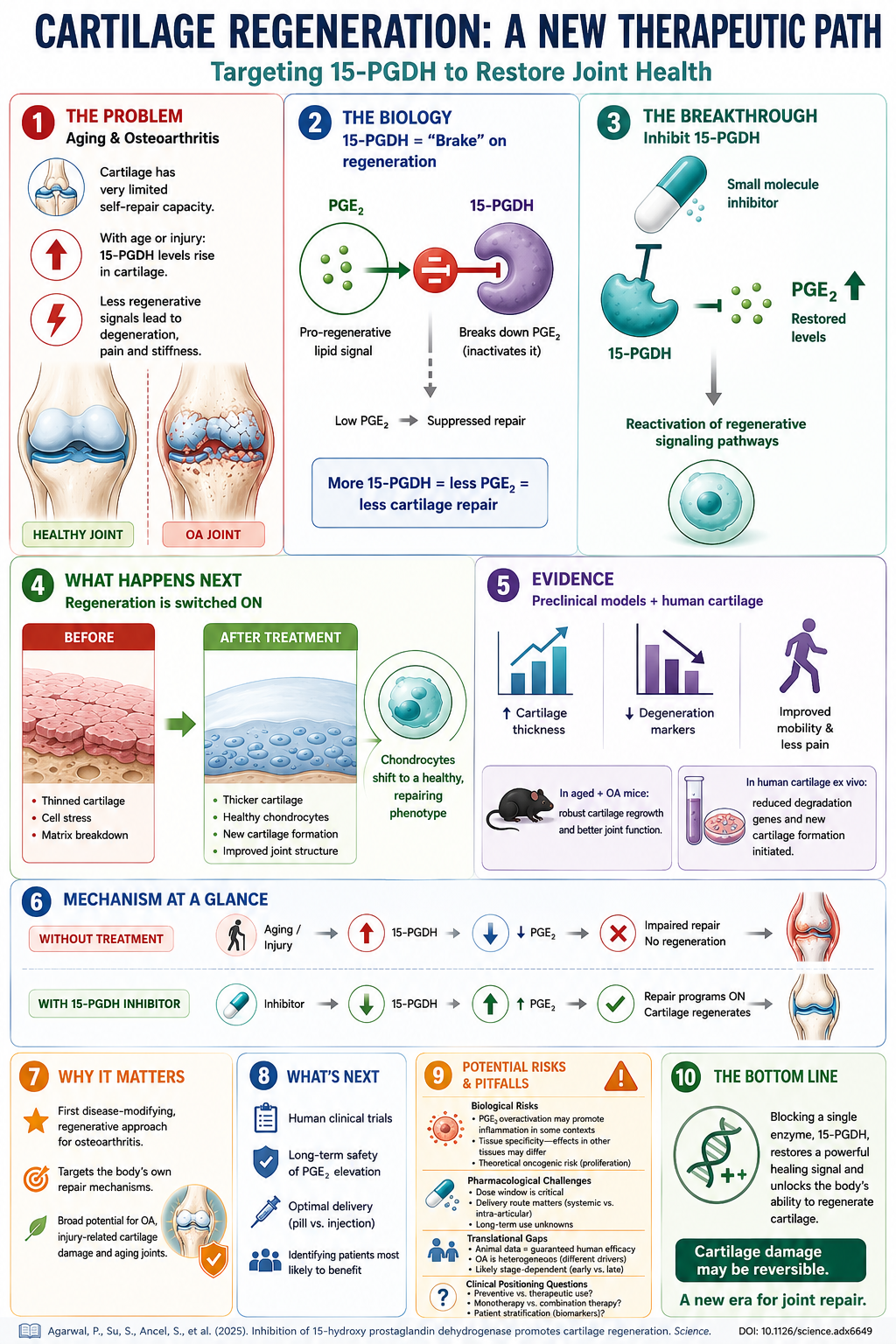
The Lipid Signal: Prostaglandin E2
Prostaglandins are lipid mediators derived from arachidonic acid — the same fatty acid pathway that produces the inflammatory signals that aspirin and ibuprofen block. Prostaglandin E2 (PGE2) specifically is well known for its role in pain and inflammation. But it also has a lesser-known anabolic role: it can stimulate cartilage-producing cells (chondrocytes) to regenerate tissue.
The Stanford team discovered that an enzyme called 15-PGDH (15-hydroxy prostaglandin dehydrogenase) — which breaks down PGE2 — is dramatically upregulated in the articular cartilage of aged or injured joints. In other words, as joints age or get damaged, they ramp up the machinery that destroys a regenerative lipid signal precisely when they need it most.
Singla M, Wang YX, Monti E et al. "Inhibition of 15-hydroxy prostaglandin dehydrogenase promotes cartilage regeneration." Science 391, 1053–1062 (2026). DOI: 10.1126/science.adx6649
The Experiment — and the Result
When the team inhibited 15-PGDH with a small molecule inhibitor — either systemically or injected directly into the joint — the results were striking: articular cartilage regenerated, and osteoarthritis-associated pain was reduced in mouse models of both aging and injury.
The mechanism: blocking 15-PGDH allows PGE2 to accumulate locally in the joint, where it reprograms damaged chondrocytes back toward a tissue-building phenotype instead of a degenerative one.
Why This Is a Big Deal
This isn't just another anti-inflammatory approach. Inhibiting 15-PGDH doesn't suppress PGE2 everywhere (which is what NSAIDs do, causing GI side effects) — it preserves a local regenerative signal specifically in damaged cartilage.
It also reframes how we think about prostaglandins. For decades, they've been cast as villains in joint disease — things to suppress with ibuprofen or steroids. This work shows that at least one prostaglandin, in the right context, is exactly what the joint needs to heal.
The broader lesson is one that runs through all of lipid biology: context matters. The same lipid mediator can be inflammatory in one setting and regenerative in another. The therapeutic opportunity lies in understanding — and preserving — the right signal in the right place.
Potential Risks and Pitfalls
As with any promising preclinical finding, the path to human therapy requires navigating real challenges:
What's Next
Blocking a single enzyme — 15-PGDH — restores a powerful healing signal and unlocks the body's ability to regenerate cartilage. If this translates to humans, it would represent the first disease-modifying, regenerative approach for osteoarthritis. Cartilage damage may be reversible. A new era for joint repair may be beginning.